Aorta
Endovascular
Sub occluding aortic thrombosis with claudication pain
Analyze the case of abdominal aortic stenosis in a 72-year-old male patient and discuss the appropriate treatment and the right choice of device.

Hospital: Paris Saint-Joseph, France
Part I - Case presentation
- The patient was a 72-year-old male with bilateral intermittent claudication 150 m
- He presented with several risk factors: dyslipidemia, diabetes, obesity (BMI 32)
- He also had a medical history of coronaropathy disease and open radical protastectomy.
Pre op CT scan
Part II - Treatment
Endovascular repair was chosen with CERAB technique.
The aortic diameter was 18 mm at the renal arteries level and the aortic bifurcation. The distance between the renal arteries and the bifurcation was 95 mm.
We made the choice of neglecting the IMA and the right accessory renal artery to achieve an extensive repair of the occluding and dissected lesion.
Procedure:
- Local anesthesia and sedation.
- Bilateral CFA punctures. Percutaneous pre-closing technique of the right access (Proglide).
- Deployment of an Endurant iliac extension 20 x 20 x 82 mm (Medtronic) 16F into the aorta below the renal arteries.
- Post-dilatation, using a Cook Coda Balloon catheter.
- Covered kissing stents using 2 Bentley Begraft stents 9 x 57 mm
- Each stents was extended with a Bentley Begraft stent 10 x 27 mm
- Kissing balloon post dilatation (10 x 40mm POBA).
Discharge on day 1 with no complications
Initial angiography
Final angiography
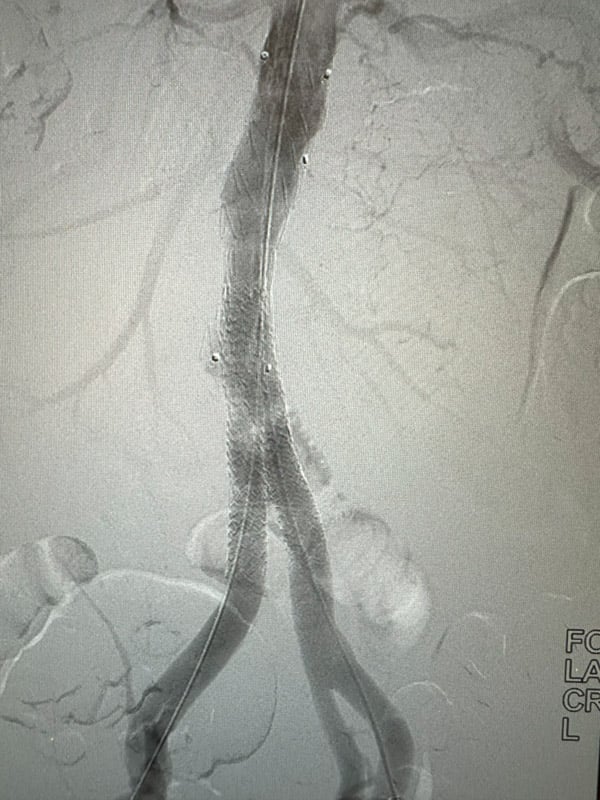
Final angiography
Take home messages
- Think outside the box! A device may be used in different indications
- Extensive repair of the aorta allows a high patency rate over the mid and long terms.
Get the latest clinical cases and breaking news delivered straight to your inbox!
